
准入是医疗集团领导人的战略重点, 但他们往往缺乏衡量自己表现的能力. Leaders juggle a variety of static reports about time to appointment or third next available, 但这些信息很少是可操作的,而且往往是不准确的.
相反,应该从供给和需求的角度来评估获取情况. 在这种情况下, 需求代表寻求新患者预约的独特患者, and supply indicates the practice’s capacity to accommodate appointments within a patient’s desired time frame. 通过持续地评估一个实践在供给和需求之间达到平衡的过程, 它可以实现更大的访问, 这就导致了增长, 财务可持续性和患者满意度.
在这个供需方程中, 医疗集团对供应有更大的控制权, 根据提供商容量来衡量. 因此, practices should begin their access journey by properly assessing and evaluating their providers’ capacity to see patients. Outlined below are three key tactics for evaluating and improving capacity to drive an access strategy:
- 分析bet8网站备用的临床时间
- 检查临床时间和生产力之间的关系
- 优化关键容量驱动因素.
分析bet8网站备用的临床时间
Medical groups tend to focus on benchmarking provider compensation and productivity; however, it can be challenging to understand whether a provider is working to his or her full capacity. This is particularly relevant for specialists whose clinical work occurs in a variety of settings. 分析提供商容量是确保访问可用的关键步骤. 在考虑招聘其他供应商之前, 评估是否可以利用现有资源增加供应.
了解当前提供商的能力, compare each provider’s actual worked hours to contracted or expected number of hours using the following steps:
1. 如果没有写入提供商合同, set a standard expectation for the number of patient-facing hours a full-time clinical provider should work, 根据每个提供者的临床努力进行调整. 例如, your institution may determine that 32 hours per week is consistent with a full-time provider, 允许每半天的病人就诊时间有一小时的行政时间. 制定每年的标准工作周数, 比如47, 每年有五周的假期.
These metrics enable you to calculate that a full-time clinical provider should be scheduled to work 1,每年504小时(每周32小时x每年47周). 同样,0.90名临床全职bet8网站备用每年工作1,354小时(1,504小时× 0小时).90立方英尺).
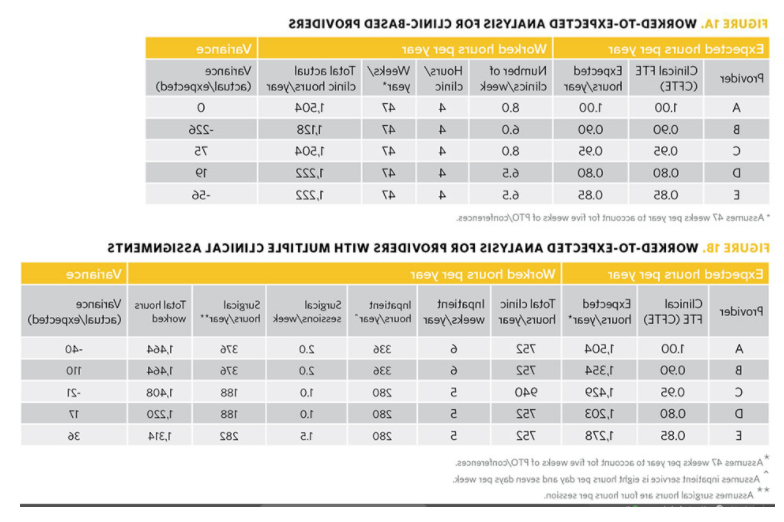
2. 量化每个供应商的实际工作时间. Depending on the specialty and type of work, the effort required to calculate this will vary. 包括在诊所的时间, 执行程序或手术, 阅读影像学研究并提供住院治疗. A primary care provider who works exclusively in a clinic setting would be straightforward to quantify, 如图1A所示. A procedural subspecialist who spends time at multiple clinical locations may be more complex to quantify, 如图1B所示. 在计算这些小时的时候, 计算所有实际工作时间是很重要的, 而不是“计划好的”时间, 哪一个可能会被未充分利用或不准确的模板所扭曲.
一旦计算出实际工作时间, compare it to the hours each provider is expected to work; this is referred to as a worked-to-expected (W:E) analysis. The W:E analysis serves as a quick guide for administrators to understand opportunity areas to improve capacity at the individual or programmatic level. It is also a useful tool in beginning discussions regarding provider time spent in clinical settings, 包括随时间变化的趋势. 例行地运行这些分析(例如.g.(每月或每季度),以调整容量,需求或时间表的变化.
检查临床时间和生产力之间的关系
一旦W:E分析完成, 将其与提供者的生产力进行比较, 如图2所示.
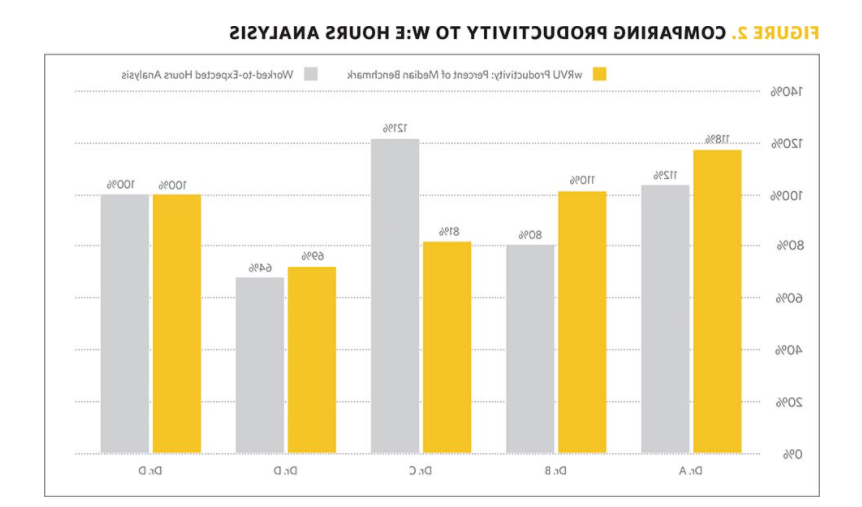
将工时分析与生产率分析进行比较.g., wRVUs as a percentage of industry median) can reveal opportunities to improve provider capacity, 因此, 病人的访问. In comparing these data points, one of four scenarios will emerge, as depicted in Figure 3:
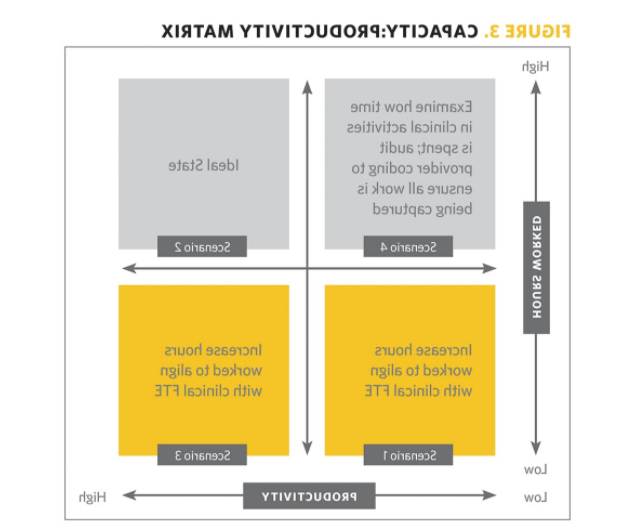
- W:E和生产力的一致性: Often a provider’s productivity performance is related to the number of clinical hours he or she works, 如下所述.
- W:工作时间低,生产力也低(场景1):在这个场景中, 提供者的工作时间应增加,以配合他或她的CFTE, 假设生产率也会提高.
- W:工作时间长,生产力也高(场景2): This is likely the ideal scenario and may not involve any action; however, leadership and the provider should be aware of risk of burnout and proactively intervene as appropriate.
- W:E和生产力的错位: While it is reasonable to assume that a provider working sufficient clinical hours will have appropriately aligned productivity metrics, 情况并非总是如此, 如下所述.
- W:工作时间短,但生产率高(场景3):在这种情况下,提供者可能效率很高, 或者他们可能比同龄人从事更多高收益的活动, 内部或外部组织. Examine these providers in the context of their colleagues to understand whether any practice nuances account for this misalignment of work hours and productivity. 例如, a pulmonary provider who subspecializes in sleep medicine may require a modified productivity benchmark.
This scenario may call for realigning benchmarks or spreading work more evenly among members of the specialty. If a provider’s clinical hours are below the expected target, clinical time should be increased. 在大多数医疗团体中, high productivity should not give providers a free pass to work fewer hours than what they are contracted. - W:工作时间长但生产率低(场景4):进一步详细检查提供者的临床时间是如何使用的, 并确保正确捕捉临床活动, 包括计费. 一些常见的不对齐区域包括:
- 提供者安排了门诊,但阻塞了不可用的时间.
- 需求很低,供应商也有空缺.
- 提供者的访问持续时间太长,其复杂性.
- 提供者的时间没有正确计费(e).g.、底层编码、开放图表、未计费的遭遇).
- 提供者的某一方面的时间没有被计算在内.g.,进行成像读取,但不收费).
- W:工作时间短,但生产率高(场景3):在这种情况下,提供者可能效率很高, 或者他们可能比同龄人从事更多高收益的活动, 内部或外部组织. Examine these providers in the context of their colleagues to understand whether any practice nuances account for this misalignment of work hours and productivity. 例如, a pulmonary provider who subspecializes in sleep medicine may require a modified productivity benchmark.
优化关键容量驱动
Even providers who are productive and working sufficient hours should focus on drivers that affect the practice’s overall access strategy. Key components that can help providers understand practice capacity and access include new patient ratio, 访问时长和转化率.
新增患者比例
生产力和访问度量并不总是一致的, and sometimes highly productive providers may be spending time on activities that don’t support the practice’s access mission. 例如, a provider who prefers to obtain wRVUs by treating two established patients instead of one new patient in the same amount of time is not prioritizing access. 在设计医护人员时间表时,应考虑到适当的新患者比例, 为新患者提供专门的预约时间. The ratio of new to return visits will vary: surgical and procedural practices should see up to a 50% new patient ratio, 而医学实践将看到更少, and primary care will see closer to 10% to 20% to align with the longitudinal care they provide.
访问的长度
The duration of appointments also has a significant impact on access and provider productivity without affecting the hours a provider works. The average visit length will vary by specialty and the amount of support provided by nurses, residents or advanced practice providers working alongside the provider; however, 减少访问次数将对访问产生直接和积极的影响. 例如, 如果提供者通常安排新患者就诊60分钟, 将每次访问减少到40分钟将使访问次数增加50%.
转化率
除了新的病人比例, 新患者对关键程序或手术的比例是一个重要的准入指标. 例如, heart surgeons who are expected to perform 200 open-heart surgeries per year will benefit from knowing their conversion rates between new patients and surgeries. 如果每一个手术平均有两个新病人就诊, this surgeon would need to provide timely access for at least 400 new patients per year to yield the desired surgical volume.
访问类型的持续时间经常是一个有争议的问题, but providers must understand that the duration is intended to be the average amount of time the provider needs to be present for the visit. Practices often make the mistake of including any pre- or post-work required for the patient’s appointment (e.g., 病史和体格, 结帐过程), 但这占用了提供商太多的时间,降低了容量. 访问时间通常是按照“最坏情况”设计的,提供者和管理人员试图解释病人最长的就诊时间, 不是平均花费的时间.
增强改善获取的能力
改善患者可及性是一项财政、战略和业务上的当务之急. 在考虑供求平衡时, 医疗集团可以专注于他们最能控制的事情:供应, 或者提供商能力. 因为医疗bet8娱乐提供者是医疗集团最有价值的资产, 对他们时代的彻底分析, 生产力和效率应该经常进行. 通过评估能力, 管理人员能够确定当前的提供者时间是否被最大化了. Only when it is optimized should additional providers be hired as a means of further expansion. 现在比以往任何时候都重要, 实践必须关注其财务可持续性, 而对患者访问的周到管理是这个难题的关键部分.
萨拉·特利, 工商管理硕士, 参谋长, Rush University Medical Center; Michelle Hirschman, 工商管理硕士, bet8娱乐线路管理员, Rush University Medical Center; and 史蒂夫·麦克米伦, 尼古拉斯, 高级经理, 心电管理顾问
2020年9月1日发布